

This piece maps how peptides and steroids are actually regulated. It does not explain how to obtain anabolic steroids, which remain controlled substances. Every legal or clinical claim below is sourced, so you can check my math and my citations yourself.
I run numbers for a living, so when a topic gets fuzzy I try to turn it into a table. “Are peptides legal” is one of those questions that resists a single answer, and most of the confusion online comes from smashing three separate questions into one. So let’s separate them, score each substance against each one, and see what the scorecard actually looks like.
The three questions: Is it a controlled substance? Does it require a prescription? Would it get a tested athlete disqualified? Three yes/no axes. Once you run steroids and peptides through all three, the “legal or not” confusion mostly clears up.


Question one: controlled substance, yes or no
Steroids: yes, cleanly. Anabolic-androgenic steroids sit in Schedule III of the U.S. controlled-substance schedule, the same tier as testosterone and ketamine, a classification meant to signal intermediate abuse potential, above Schedule IV, below Schedule II [1]. That’s a hard legal line, not a vibe. Manufacture, distribution, and possession are federally governed, and there’s no “research use only” workaround, because that label simply doesn’t apply to anything already on a schedule.
Peptides: mostly no. Most peptides never touch a controlled-substance schedule at all. But that’s a smaller win than it sounds like, because “not controlled” is not the same as “legal for you to buy and inject.” That’s question two, and it’s where the real split happens.
Question two: prescription and FDA status
This is where I want a table, because two peptides can look identical on a label and sit on opposite sides of the law.
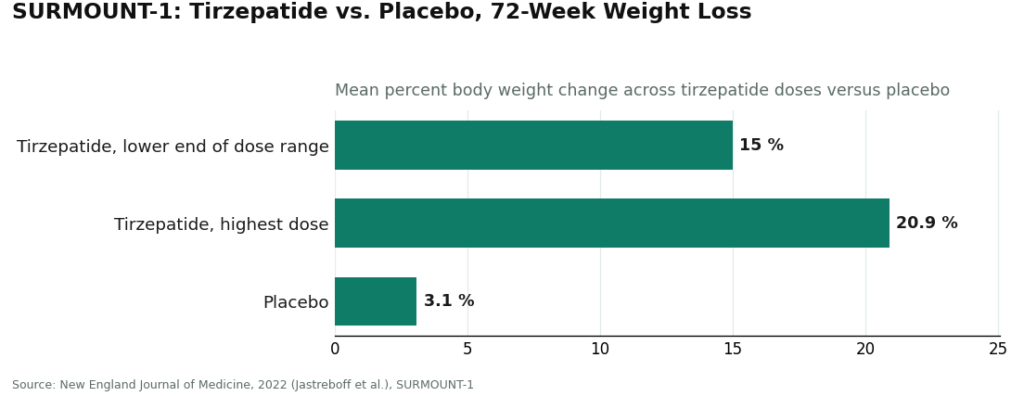
FDA-approved, prescription route: Semaglutide and tirzepatide are peptides by structure, classed as incretin-based agents that boost insulin secretion, suppress glucagon, slow gastric emptying, and increase satiety [2]. They’re legal with a prescription, and the trial data behind them is substantial. In SURMOUNT-1, published in the New England Journal of Medicine, tirzepatide produced average weight loss of 15.0% to 20.9% across doses over 72 weeks, versus 3.1% on placebo [3].
I’ll do the quick math myself: at the top dose, that’s roughly seven times the placebo effect (20.9 divided by 3.1). That’s not a new number, just a ratio built from the two numbers already in the trial, and it’s the single figure I’d point to if someone asked me “does this actually work?” It’s the cleanest evidence-backed number in the whole peptide category.
“Research use only,” everything else: A huge share of peptides sold online carry the words “not for human consumption” right on the label. That phrase gets misread constantly as a wink-wink gray-market disclaimer. It isn’t. It’s the entire legal foundation the seller is standing on. Sell a chemical for lab research, you’re in one regulatory bucket. Market it for a person to inject, you’ve become an unapproved drug. So sellers write the label carefully, and buyers who read past it are the ones taking on the risk.
What that means in practical terms: no FDA review of identity, strength, or purity. No clinician evaluating whether it’s right for you. No pharmacy. No recall mechanism if a vial turns out mislabeled or contaminated. The sticker isn’t a green light, it’s a legal fence the seller built for themselves.
So the peptide column of my table has two very different rows, not one:
| Category | Controlled substance? | Legal to use? | FDA quality review? |
|---|---|---|---|
| Anabolic steroids | Yes, Schedule III [1] | Prescription only | N/A, controlled |
| FDA-approved peptides (semaglutide, tirzepatide) | No | Yes, with prescription [2][3] | Yes |
| “Research use only” peptides | Mostly no | Legally gray for personal use | No |
Same word, “peptide,” two completely different legal rows. That’s the whole confusion in one table.
Question three: would it flag a drug test
Anti-doping rules run on a separate ledger entirely, and this is the one competitive athletes trip over. It doesn’t matter whether something is legal to buy or legal to prescribe. It matters whether it’s on the list.
Under the 2026 anti-doping rules, the S1 anabolic agents category covers anabolic-androgenic steroids, and the 2026 language was specifically clarified to state that esters of prohibited anabolic agents are included too, citing testosterone cypionate and testosterone propionate by name [4]. SARMs land in the same S1 bucket. All of it is prohibited at all times, in and out of competition.
Many peptides and growth factors are prohibited as well. So for a tested athlete: a “research use only” sticker gives zero legal cover here, and a real prescription only helps if it’s paired with a therapeutic use exemption. The bottle’s wording, and how you got it, are both irrelevant to whether it’s banned.
Reassembling the scorecard
Run it all the way through and the picture is sharper than any one piece alone:
- Steroids: controlled (yes), prescription-only with no legal workaround, banned in sport at all times [1][4]. Three yeses on the “restricted” side, no soft version exists.
- FDA-approved peptides: not controlled, legal with a prescription, backed by real trial numbers like the SURMOUNT-1 figures above [2][3]. This is the one row where “legal and studied” both check out.
- Research-use peptides: not controlled, legally gray for personal use, unreviewed for quality, and frequently banned in sport regardless. This row has the most caveats and the least data.
“Are peptides legal” doesn’t have one answer because peptides aren’t one category. That’s not a dodge, that’s the honest scorecard.
Where the supervised, legal lane fits
If someone wants to stay on the documented, prescription side of this whole comparison, the structure is straightforward: licensed clinician, prescription where appropriate, licensed pharmacy dispensing it. That’s the entire difference between an approved or properly compounded medication used under supervision and an unlabeled powder ordered off a research-chemical site.
FormBlends is a telehealth provider that operates on that supervised, prescription side of the line I’ve been drawing here. I’m citing it as an example of what the legal, supervised structure looks like in practice, not as a product recommendation and not as a ranking, there’s nothing to buy through this article. It sits firmly on the prescription-peptide row of my table above. It is not, and does not claim to be, a route to controlled anabolic steroids.
One caveat I want on the record because it changes the risk math: a lot of what runs through this supervised route is compounded medication, and compounded drugs are not FDA-approved finished products. The FDA hasn’t evaluated them for safety, effectiveness, or quality the way it does an approved brand drug. Supervision adds a clinical-oversight layer on top, it doesn’t convert a compounded preparation into an approved one. Any provider worth trusting says that plainly instead of burying it.
The pick, if you’re asking me
If I had to boil the scorecard into one line: steroids are a closed door (controlled, prescription-bound, banned), research-use peptides are an open door with no inspector standing behind it, and FDA-approved peptides like the GLP-1 drugs are the only row where you get both legal clarity and real trial numbers behind the claim. That third row is where the actual evidence lives. The other two rows are where the internet’s confusion lives.
Are peptides and steroids actually legal to buy in 2026?
Run it through the three-question framework and the answer depends on which compound and which country. In the U.S., anabolic steroids are Schedule III controlled substances, so possession without a valid prescription is a federal offense, full stop. Peptides split into rows: something like BPC-157 has no approved human-drug status and sits in a gray zone, while tesamorelin is FDA-approved and fully legal with a prescription. Gray-zone isn’t a synonym for safe.
What’s the real cost gap between peptides and steroids?
Prescription anabolic steroids through a legitimate pharmacy run roughly $30 to several hundred dollars a month depending on the compound and dose. Peptides show a similarly wide spread: FDA-approved versions prescribed through a physician-supervised compounding pharmacy like FormBlends typically cost more than black-market vials, and that premium is buying tested purity and legal accountability, not markup for its own sake. Research-chemical peptides are cheap precisely because nobody’s verifying what’s actually in the vial.
Which wins on body composition, peptides or steroids?
Steroids generally move faster and produce more pronounced muscle gains because they bind androgen receptors directly and drive protein synthesis hard. Growth-hormone-stimulating peptides like CJC-1295 or ipamorelin tend to shift body composition more gradually, with a different side-effect profile. I wouldn’t call either universally “better,” because health status, goals, and risk tolerance change the math for every individual, and the evidence base for many peptides in otherwise healthy adults is thin next to decades of steroid research.
Where do people actually source these, and what’s the risk by channel?
Prescription steroids come through licensed pharmacies with a doctor’s oversight, the only legal route in the U.S. Peptides without approved status are commonly sourced from research-chemical sites or overseas suppliers, and independent testing on those products regularly turns up contamination, wrong concentrations, or outright substitute compounds. Buying either substance from an unverified source stacks purity risk directly on top of whatever legal exposure already exists, and there’s no recourse if the vial turns out to be something other than advertised.
References
- Anabolic steroids are Schedule III controlled substances, the same tier as testosterone and ketamine, reflecting intermediate abuse potential. Drug Scheduling, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK557426/
- GLP-1 receptor agonists (e.g., semaglutide) are incretin-based peptide agents that increase insulin secretion, suppress glucagon, delay gastric emptying, and increase satiety. Glucagon-Like Peptide-1 Receptor Agonists, StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK551568/
- SURMOUNT-1 tirzepatide trial: mean weight loss of 15.0% to 20.9% across doses vs 3.1% placebo at 72 weeks. New England Journal of Medicine, 2022 (Jastreboff et al.).
- 2026 anti-doping rules: S1 anabolic agents (anabolic-androgenic steroids and SARMs) are prohibited, with clarification that esters of prohibited anabolic agents are included (e.g., testosterone cypionate, testosterone propionate). USADA Athlete Advisory on the 2026 WADA Prohibited List.
This does not diagnose, treat, or prescribe, and it is not a substitute for a licensed clinician or attorney. Some medications described here are prescription-only, and many are compounded preparations that are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality. Talk to a licensed clinician before starting any of this. Nothing here explains how to obtain anabolic steroids, which are controlled substances.
Written by Aisha Eriksen, reporting fellow. Grounding every claim in the sources linked here. Last reviewed June 2026.
Not professional medical advice. Speak with your healthcare provider before making a change.



